
Dr. Baxter is also the founder of The Alabama Tongue-Tie Center, next door to Shelby Pediatric Dentistry, where he uses advanced laser technology to fully release your child’s lip- or tongue-tie in a gentle, 15-second procedure.
One tiny string can be a serious pest.
Does your infant…
Struggle to nurse or take a bottle?
Have milk leaking out of his mouth while eating?
Make clicking or smacking noises when eating?
Have slow or poor weight gain?
Have reflux of colic symptoms?
Have lots of gas or experience frequent fussiness?
Does your older child…
Have restless sleep?
Speak softly (mumble) or struggle to be understood?
Have slow or picky eating?
Choke or gag on liquids or foods?
Have a strong gag reflex?
Have a speech delay?
Grind teeth at night, snore, or sleep with his mouth open?
If so, your child may have a tongue- or lip-tie.
While they aren’t usually life-threatening, oral restrictions can mean a lot of unnecessary limitations to your child’s life. At The Alabama Tongue-Tie Center, we believe your child should never be held back
by something so completely treatable.
Help your child eat, sleep, and speak better.


Peek inside Dr. Baxter’s best-selling book.
Tongue-Tied: How a Tiny String Under the Tongue Impacts Nursing, Speech, Feeding, and More is an exhaustive and informative guide to this misunderstood affliction. Along with a team of medical specialists, author Dr. Richard Baxter demystifies tongue-ties and spells out how this condition can be treated safely, comfortably, and comprehensively.
FAQ
Is your infant struggling to nurse?
A new baby with a too tight tongue and/or lip frenum can have trouble sucking and may have poor weight gain. If they cannot make a good seal on the nipple, they may swallow air, causing gas, colic, and reflux or spitting up. You may hear clicking noises when the baby is taking the breast or a bottle.
A nursing mother who experiences significant pain while nursing or whose baby has trouble latching on should have her child evaluated for tongue- and lip-tie. It can also cause thrush, mastitis, nipple blanching, bleeding, or cracking in the mother and the baby may be unable to hold a pacifier. The mother often reports, it’s a “full-time job” just to feed her baby, because he or she is constantly hungry, not getting enough milk, and spitting up often.
Although it can be overlooked or dismissed by other medical professionals, a tongue- and/or lip-tie can very often be an underlying cause of feeding problems that not only affect a child’s weight gain but lead many mothers to abandon breastfeeding altogether.
Very often, after releasing the tongue and/or lip, mothers report immediate relief of pain and a deeper latch. The symptoms of reflux and colic almost disappear and weight gain occurs rapidly. The sooner the tie is addressed the better the child will learn to function with the increased range of motion.
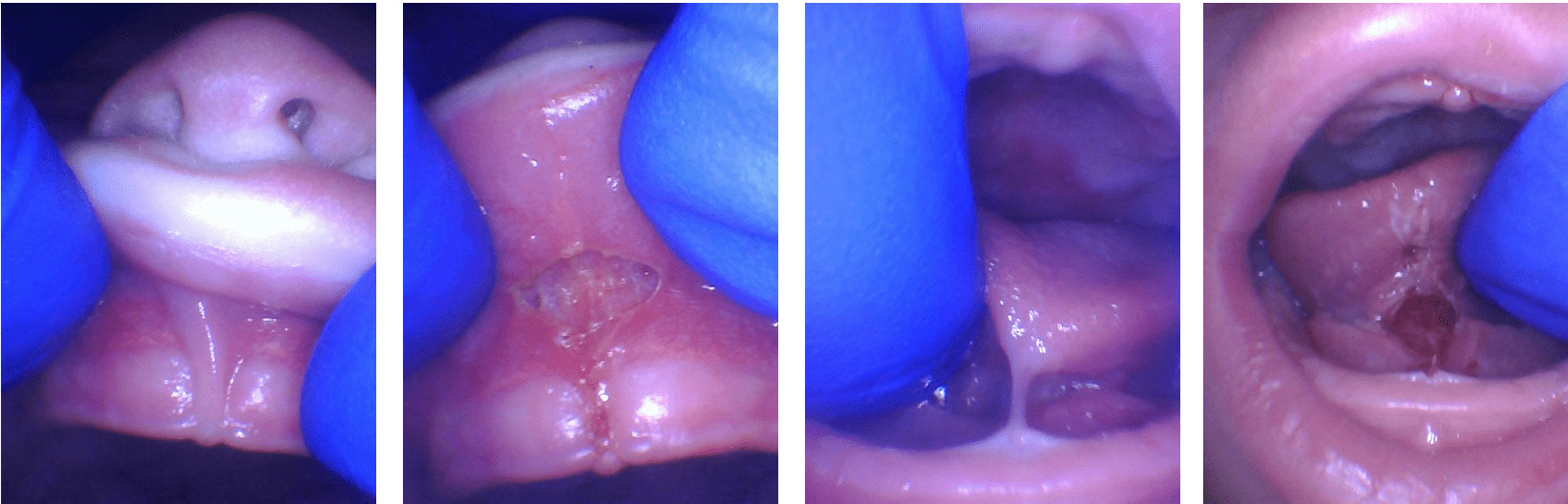
Notice in the photo how the lip will not roll outward when lifted. After the release, it fully lifts to the nose. The tongue is held down all the way to the gum. This is a severe tongue-tie, but even less severe ties can cause similar problems. Afterward, notice how high the tongue can lift with greater mobility.
A posterior tongue-tie could also be causing the problem.
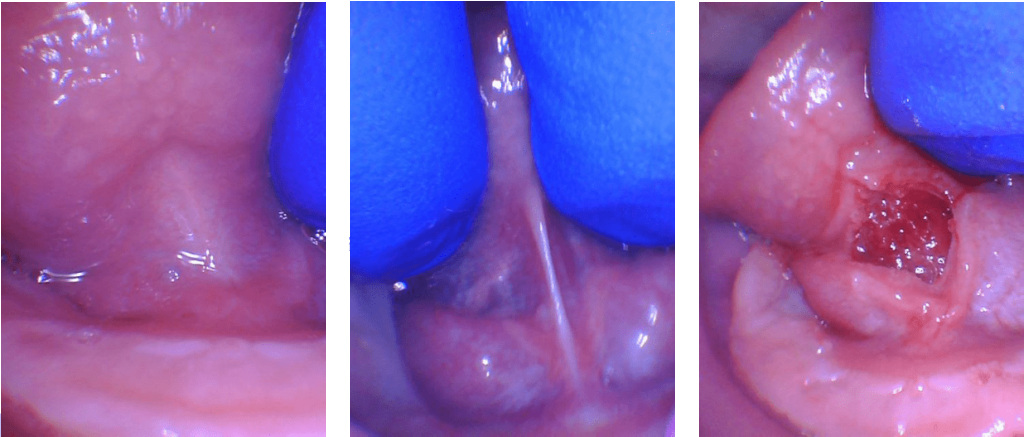
This is a photo of a posterior tongue-tie. If a baby has symptoms of a tongue-tie (not gaining weight, poor latch, clicking when nursing, gumming the nipple, painful nursing, reflux, gassy, etc.) and there is not an obvious string, it is very likely a posterior tongue-tie. This is a hidden tie that is felt easily but is very often overlooked by medical professionals that have not been trained to identify it.
Notice the picture on the left. It looks like there is no problem, but the baby and mother are having lots of difficulty nursing. When the tongue is lifted with two fingers, notice the tight tissue that pops up. After release, a diamond shape shows that the tongue-tie release was complete and the baby instantly nursed better and mom noticed a huge difference in the depth and quality of the latch. The baby took twice as much milk in half the time they normally spent nursing.
Does your toddler or older child struggle with speaking, eating, or sleeping?
Speech:
While the tongue is remarkably able to compensate and some children have no speech impediments due to tongue-tie, many continue to struggle. By the age of three, speech problems, especially articulation of the sounds L, R, T, D, N, TH, SH, and Z may be noticeable. An evaluation may be needed if more than half of a four-year-old child’s speech is not understood outside of the family circle. The child with a tongue-tie may have a lisp or have difficulty speaking when tired. It can also lead to sleep apnea, mouth breathing, other airway issues and cause difficulty chewing and swallowing food. It can be difficult for older children and adults to “roll” their Rs, as necessary in Spanish.
Speech delay has not been associated with tongue-tie in research studies (yet!), however, we have seen that many tongue-tied children do have a speech delay, and begin saying new words even just hours or days after the release! One child said four new words the same day as the procedure. Another had 29 new words the week of the procedure (and only 10 to begin with). There is no guarantee that every child will have immediate results, but we often see this type of drastic improvement.
Although there is no obvious way to tell in infancy which children with tongue-tie will have speech, feeding, or sleep difficulties later, the following characteristics are common:
- Heart-shaped tip of the tongue, or a thick band of fibers under the tongue.
- Inability to touch the roof of the mouth with the tongue, or get close (this is the best test!).
- Difficulty moving the tongue from side to side.
Feeding
Children that are tongue-tied often have eating issues from infancy, such as trouble nursing or taking a bottle. When transitioning to solid foods, they may choke, gag, or spit food out and even refuse to wean. In childhood, these eating difficulties can persist and are evidenced by only eating small amounts of food (or “grazing” throughout the day) and slow eating, often being the last to finish at mealtimes.
These issues are due to the fact that difficulty swallowing can lead to distraction. Pickiness, especially with textures, can often occur, as certain types of food are challenging to swallow. Soft, mushy foods and meats are typically the most difficult, but children can struggle with chewy and hard foods as well.
In our experience, we have seen children with tongue-ties (even “hidden” posterior ties) improve within hours or days of the release. Often parents have been searching for years to figure out why their child cannot eat well. All along, the thick, tight string under the tongue was preventing normal tongue mobility and swallowing.
Sadly, training on tongue-ties is lacking in medical and dental programs, so most healthcare providers are not up-to-date on the latest diagnostic techniques and procedures. Even if your child has been told that he or she “does not have a tongue-tie” but exhibits all the symptoms, there is a good chance it is a posterior tongue-tie and should be evaluated.
Certainly not every feeding problem is a result of a tongue-tie, but very often there is a connection, and this simple solution can be easily overlooked.
Sleep and Tonsils
A tongue-tied child will often grind his or her teeth at night, snore or experience other sleep-disordered breathing problems. Releasing a tongue-tie can help a child to sleep more soundly because the tongue will be able to rest on the palate (where it is supposed to rest) rather than falling back to narrow or block the child’s airways. Sleep-disordered breathing can cause frequent waking, restlessness, bed-wetting, not waking up refreshed and accompanying difficulty focusing (which is sometimes misdiagnosed as ADD or ADHD).
Because multiple factors contribute to the problem, such as large tonsils and adenoids, a narrow palate and tongue-tie, often a child will be seen by multiple specialists to try to remedy the problem. In addition, children with tongue-ties often have a history of multiple ear infections, needing ear tubes, and having tonsils and adenoids removed. All of these can be complicated by the mouth-breathing that frequently occurs in tongue-tied individuals, due to the low resting posture of the tongue. We have found that when there is a tongue-tie, sleep often improves dramatically after a simple in-office procedure.
Dental
For older children with a lip-tie, it is common to have a gap between the two front teeth. This often closes if the frenum is removed (typically done before 18 months old or around age 8, when the permanent teeth erupt). The tongue-tie can also pull against the gums on the back of the teeth and cause recession. The tight lip-tie may trap food and make it difficult to remove plaque from the front teeth, leading to cavities.
What is a tongue-tie or lip-tie?
Most of us think of tongue-tie as a situation we find ourselves in when we are too excited to speak. Actually, tongue-tie is the non-medical term for a relatively common physical condition that limits the use of the tongue, ankyloglossia. Lip-tie is a condition where the upper lip cannot be curled or moved normally.
Before we are born, a strong cord of tissue that guides the development of mouth structures, called a frenum is positioned in the center of the mouth. There is also one located under the upper lip. As we develop in the womb, these frena are supposed to recede and thin. The lingual (tongue) and labial (lip) frena are visible and easily felt if you look in the mirror under your tongue and lip. Everyone has these, but in some people, one or both can be especially tight or fail to recede and may cause tongue/lip mobility problems.
The tongue and lip are a very complex group of muscles and are important for all oral functions. For this reason, having a tongue-tie can lead to nursing, feeding, dental, sleep, or speech problems, which may be serious in some individuals. Problems can even persist into adulthood with migraines, neck pain, shoulder pain, and speech problems.
Does your child have a lip- or tongue-tie?
Identifying tongue- and lip-ties is not taught in medical school, dental school, or residency – so even when I was two weeks away from becoming a pediatric dentist, I had never heard about it, except in passing, and as a rare condition (when in fact, it affects 1 in 4 people, hardly rare!).
There are many children who have difficulties related to tongue-ties and lip-ties, but unfortunately, they’re often not identified until later in life. They can cause various nursing difficulties, failure to gain weight, speech difficulties, feeding difficulties, sleep issues, and cavities.
Even though we are a dental office, we take the whole mouth into consideration, not just the teeth. We are proud to have helped countless children with tongue-tie or lip-tie issues – from 1-week-old babies having difficulty gaining weight, to 1-year-olds with brushing difficulty due to restricted lip movement, to 14-year-olds with speech impediments.
If your baby is having difficulty nursing or you are experiencing pain while breastfeeding, your child may have a tongue- or lip-tie. Difficulty taking a bottle (clicking noises can be an indicator), reflux or colic, failure to gain weight appropriately, and speech issues can all be symptoms of these conditions. Often times, ties are genetic, so while the child is in for treatment, a parent realizes they also have a tongue-tie (evidenced by speech problems, migraines, reflux, etc.).
If you notice any symptoms in your child and suspect a tongue- or lip-tie, or even just want to explore the possibility and ask some questions, Dr. Baxter or one of our team members would be happy to speak with you. From his own experiences, Dr. Baxter realizes how easily this condition can go undiagnosed and how difficult it can be to live with the effects. And, the sooner a tongue or lip is released, the better the child is able to adapt to the new mobility.
How does the procedure work?
Tongue-tie and lip-tie release is a simple procedure and there are virtually no complications when using a CO2 laser and good technique. The procedure may be performed as early as a couple of days after birth and as late as 70 years old! Typically, once a problem with a tongue-tie or lip-tie has been discovered, the sooner it is addressed the better the procedure will work and the greater the outcome will be in resolving the tongue-tie symptoms.
Using a state-of-the-art dental laser, we can easily release ties in our office with minimal to no bleeding and no stitches. We have upgraded from a pen-like diode laser with a hot tip (what most “laser” dentists use) to a new LightScalpel CO2 laser that works faster, is less painful, and results in a better healing process. A lip-tie release now takes us 15 seconds and a tongue-tie release, around 10 seconds.
Children who are old enough to be anxious about the procedure receive some numbing medicine and laughing gas and usually report no pain at all. Younger children and babies usually cry more due to us working in their mouths and holding them still than from the pain.
Parents of infants are encouraged to wait in the private nursing room while we take before and after photographs and complete the quick procedure. Usually, this only takes a total of 2-3 minutes. Parents may choose to accompany children 12 months and older into the treatment room if they desire. The laser gently removes the tight tissue with virtually no bleeding and no stitches. The baby is allowed to nurse immediately after the procedure, and older children will notice an immediate difference in mobility of the tongue. Often speech is improved within a few minutes to a few weeks, but speech therapy is still needed and it is recommended to work with a myofunctional therapist for children older than 4 years of age.
We have had the pleasure of helping families from as far away as Florida, Georgia and Mississippi, and have even had patients from France, Norway and Japan. So don’t hesitate to give us a call and let us help. The Tongue-Tie Center’s phone number is 205-419-4333
Why is Dr. Baxter passionate about helping kids with tongue-ties?
This is a topic that is near and dear to my heart. I had a tongue-tie and didn’t know about it until dental school when it was partially released. Even after the partial release, I still found it difficult to pronounce “L” sounds or speak clearly and quickly. More recently, I had it fully released using the CO2 laser and find I can move my tongue more freely (touch my palate and clean my back teeth) and pronounce words with greater clarity. Afterward, I didn’t tire when reading aloud to my kids or speaking for extended periods of time.
When our twin girls were born, they had difficulty nursing and we soon realized they were both tongue-tied (it’s often genetic), and each had a top lip that was tied down to her palate. We found a dentist in Ohio that was able to complete the procedure with a laser, and later that day, they were both nursing better. We were very relieved! Our latest addition, Molly, had a tongue-tie to the tip that we noticed at her first cry. We fixed it in the office on the way home from the hospital the day after she was born, and she nursed better immediately, gaining a pound every week, for seven weeks, exclusively breastfed. She’s happy and content, and since we were armed with the right information, we were able to avoid many of the issues our twins experienced.
What are the expected results?
One important thing to understand when your child has a tongue or lip-tie revised is that improvement is not always immediate. The release of the frenum is usually just the first step. Your child will need some time to figure out what to do with the new mobility of his or her tongue or lip.
The tongue is a muscle, and it becomes used to functioning in a certain way, just like any other muscle in the body. When tongue function is restricted by a tongue-tie, the body adapts and other muscles have to help compensate. When a tongue-tie is released, the child has no muscle memory of how to use the tongue effectively without the restriction. It takes time for the brain to figure this out.
While most mothers notice an immediate improvement in their infants’ ability to nurse, it is also completely normal for this to take time. In some cases, there may even be a little regression in sucking (things get worse instead of better) for a day or two as your child’s brain tries to sort out how to use an unrestricted tongue. Sometimes, babies need chiropractic or craniosacral therapy to address other issues, such as torticollis (tight neck muscles), that can affect nursing.
Learn more about mouth restrictions in our video resource library.
The following are some helpful videos Dr. Baxter and his team have made about examining a baby for tongue-tie and lip-tie, aftercare exercises, and a video of Dr. Baxter performing the tongue-tie release procedure with the CO2 laser.
Notice there is no bleeding and no stitches are needed. It takes about 10-20 seconds, and the baby is taken immediately back to the mother in a private nursing area to feed. Often, an immediate improvement is noted in the quality of the latch, while less clicking noises are heard, more milk is taken (as assessed by our highly accurate baby scale), and less pain is experienced by the mother. It’s best to not feed your baby for an hour before the procedure so the baby is hungry and wants to nurse afterward.
We use no sedation, injections, or general anesthesia for the babies, and there is minimal to no risk when performed by a knowledgeable provider such as Dr. Baxter. Children are not sedated and don’t need general anesthesia, and we rarely even need nitrous oxide (laughing gas) as the procedure is typically easier than a dental filling.
Tongue-Tie Treatment for Infants
Tongue-Tie Treatment for Kids and Adults
Amazing Changes After a Proper Tongue-Tie Release
Trust your gut when something feels “off.”